Carpal Tunnel Syndrome is a common condition caused by compression of the median nerve as it passes through a narrow tunnel in the wrist. It can lead to tingling, numbness, and weakness in the hand, particularly at night or when using the hand for prolonged periods. Early recognition and appropriate treatment can prevent long-term nerve damage and restore normal hand function.
Carpal Tunnel Syndrome develops when swelling or thickening of the tissues within the carpal tunnel puts pressure on the median nerve. It can occur without a clear cause but is often associated with repetitive hand use, wrist arthritis, fluid retention (as in pregnancy), thyroid disease, or diabetes. It is also more common in middle-aged women and in those performing manual or computer-based work.
You experience sudden or severe hand weakness, constant numbness, or loss of thumb movement. These symptoms may indicate significant nerve compression that requires urgent medical assessment.
Call 999 for emergencies, or NHS 111 for urgent advice.
The symptoms usually begin gradually and are often intermittent at first. Many patients notice tingling or numbness at night, which can wake them from sleep and is often relieved by shaking or hanging the hand down. As the condition progresses, the numbness may persist during the day, and fine motor tasks such as fastening buttons or typing become difficult. Some patients describe pain radiating up the arm, particularly when driving or holding a phone. Weakness of pinch and grip strength can occur if the condition is left untreated.
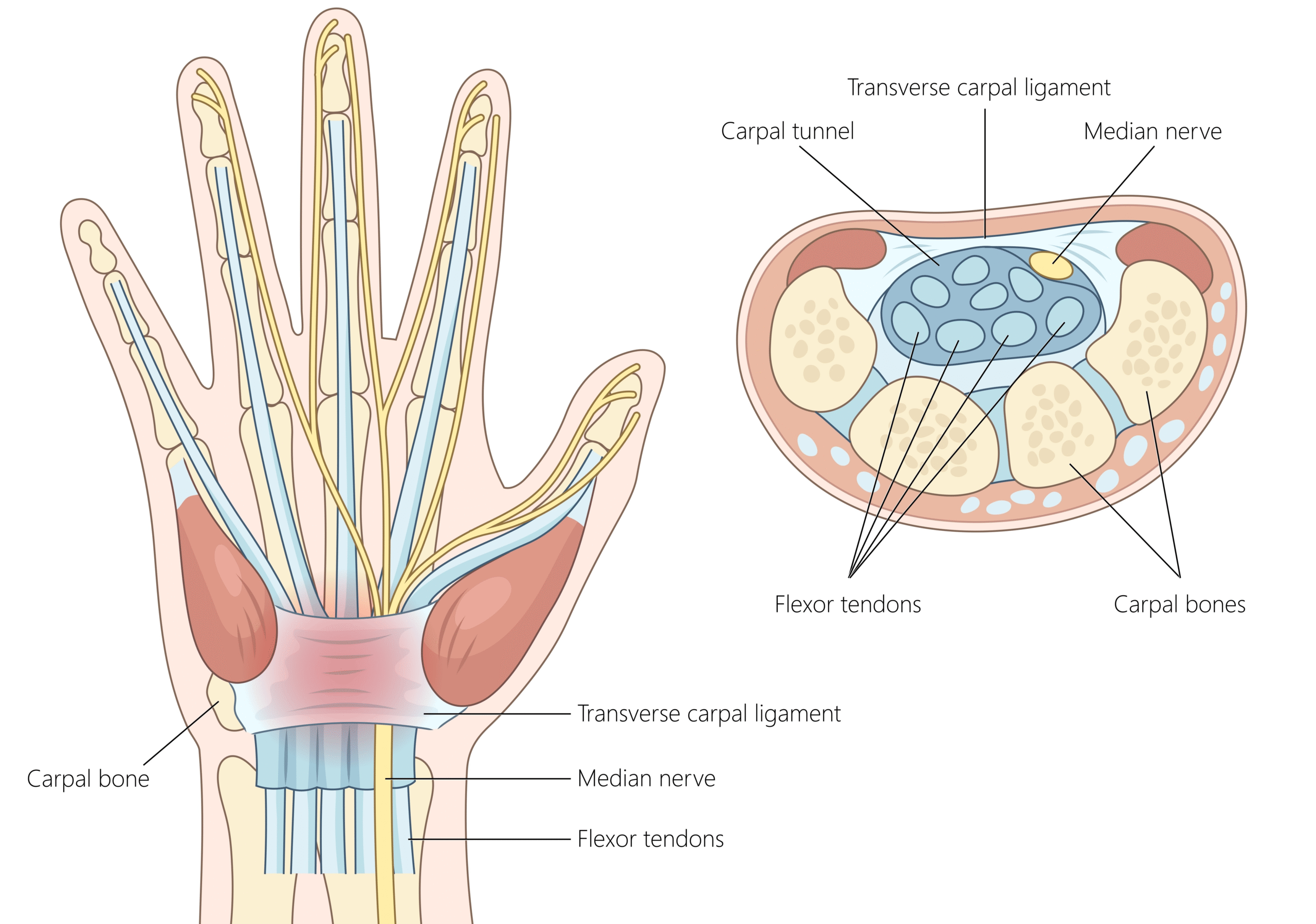
Carpal Tunnel Syndrome results from increased pressure within the carpal tunnel – a narrow space formed by the wrist bones and a thick band of tissue called the flexor retinaculum / transverse carpal ligament. Any swelling of the tendons or soft tissues within this tunnel can compress the median nerve.
Risk factors include:
In most cases, no identifiable cause is found, and the condition is considered idiopathic.
Diagnosis is primarily clinical, based on the pattern of symptoms and examination findings. Typical features include sensory changes in the median nerve distribution and weakness or wasting of the thumb muscles.
Investigations may include:
These investigations help guide whether conservative or surgical treatment is most appropriate.
Non-surgical
Mild or early cases can often be managed without surgery.
Surgical
If symptoms persist, worsen, or nerve conduction studies show significant compression, carpal tunnel release surgery may be advised. This procedure involves dividing the tight ligament roof of the tunnel to relieve pressure on the nerve. It can be performed under local anaesthetic, usually as a day-case operation, with a high success rate and rapid recovery.
Most patients notice an improvement in tingling and night pain within days of surgery, though full recovery of sensation may take weeks or months depending on the severity and duration of compression. Stitches are usually removed after 10–14 days, and light use of the hand is encouraged early.
Return to desk-based work is often possible within 1–2 weeks, while manual workers may need 3–4 weeks before resuming full duties. Follow-up is arranged to monitor wound healing, nerve recovery, and grip strength. Recurrence after successful release is rare.
You should seek urgent medical attention if you experience rapidly worsening numbness, constant tingling that does not improve with rest, or sudden weakness in thumb movement. New or severe pain, swelling, or signs of infection after surgery (such as redness, warmth, or discharge) also warrant prompt review.
Call 999 immediately or attend A&E if you have a new injury with loss of movement or sensation in the hand, rapidly spreading redness or swelling with fever, or sudden severe weakness.
Use NHS 111 for urgent same-day advice if your symptoms are getting quickly worse.
If you’re experiencing carpal tunnel syndrome or related symptoms, we can confirm the cause and tailor a plan – often starting with splints/hand therapy and exercises, with medicines, injections or surgery only where appropriate.
This page provides general information and is not a substitute for individual medical advice.
For emergencies (severe/new weakness, spreading infection, uncontrolled pain, significant injury) call 999, or use NHS 111 for urgent guidance.
Appointments:
Clinics are available at:
To book or ask a question, contact Vikki (Private Secretary):
☎ 07510 417479
✉ [email protected]
Please select your preferred site for online booking
Next to the Queen Elizabeth Hospital, Birmingham.
Convenient for Birmingham and the wider West Midlands.
Good access from the M6 and M54.
Recognised by all major insurers.
Self-pay packages available.
Convenient for patients from south Birmingham and beyond.
Insured and self-pay patients welcome.
Prefer to speak to someone?
Call my private secretary, Vikki Hibbert, on 07510 417479 or email
[email protected] for advice or to arrange an appointment.