Scaphoid Fracture / Nonunion
The scaphoid is one of the small carpal bones of the wrist, located near the base of the thumb. A scaphoid fracture commonly occurs after a fall onto an outstretched hand and can easily be missed on initial X-rays. Because the bone has a limited blood supply, untreated or delayed diagnosis can lead to poor healing or nonunion, causing persistent pain, stiffness, and long-term arthritis. Early recognition and appropriate management are vital to ensure optimal recovery and prevent complications.
Common Symptoms
- Pain and tenderness on the thumb side of the wrist after a fall
- Pain made worse by gripping or pushing up from a chair
- Swelling around the base of the thumb
- Reduced wrist motion or grip strength
- Persistent ache that fails to settle after an injury
Typical Causes
Scaphoid fractures commonly occur due to a fall onto an outstretched hand with the wrist extended or can follow a hyperextension injury e.g. goalkeeper. They are most common in young adults and athletes. Nonunion develops when the bone ends fail to heal together, often due to poor blood supply, smoking, or inadequate immobilisation.
Seek urgent help if
You have ongoing wrist pain after a fall, particularly with tenderness in the hollow at the base of the thumb (the “anatomical snuffbox”). Early diagnosis and treatment are essential to prevent long-term complications.
Call 999 for emergencies, or NHS 111 for urgent advice.
On this page:
Symptoms
The symptoms can be subtle and easily mistaken for a sprain. Most patients report pain on the radial (thumb) side of the wrist, worsened by gripping, lifting, or twisting. There may be mild swelling or bruising, but sometimes little visible deformity.
A classic finding is tenderness in the anatomical snuffbox, the small hollow between the thumb tendons on the side of the wrist. Pain on thumb movement or axial compression (pushing down on the thumb) is also typical.
In cases of delayed or missed diagnosis, patients often present weeks or months later with persistent pain, weakness, or stiffness.
Causes / Risk Factors
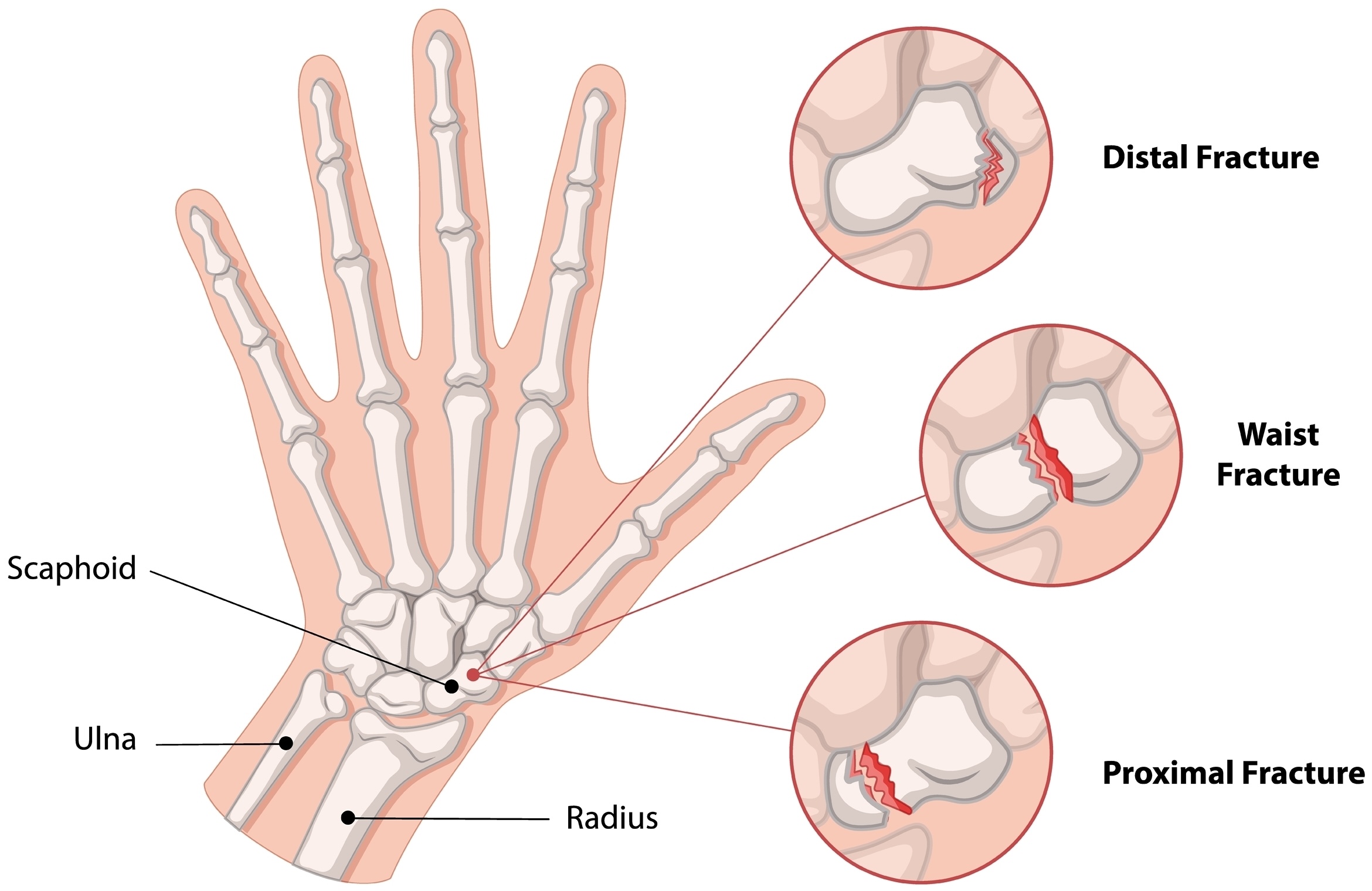
The scaphoid bone bridges the two rows of small carpal bones and plays a key role in wrist stability. Its unique shape and limited blood supply make it vulnerable to nonunion if the fracture is not promptly recognised or properly treated.
Risk factors include:
- Fall onto an outstretched hand (most common mechanism)
- High-impact sports (e.g. snowboarding, football, cycling, skateboarding)
- Delayed diagnosis or missed fracture on X-ray
- Inadequate immobilisation or premature cast removal
- Smoking (which impairs bone healing)
- Fractures through the proximal pole, where blood supply is poorest
Investigations & Diagnosis
A thorough clinical examination is essential. Tenderness in the anatomical snuffbox or over the scaphoid tubercle is highly suggestive of injury.
Investigations include:
- X-rays: initial imaging may be normal, particularly within the first few days.
- MRI scan: the gold standard for detecting occult (hidden) scaphoid fractures when X-rays are negative but suspicion remains high.
- CT scan: used to assess fracture displacement, alignment, and healing progress, particularly in cases of delayed union or nonunion.
If a scaphoid fracture is suspected but not visible on X-ray, the wrist is usually immobilised in a cast or splint until advanced imaging confirms or excludes the diagnosis.
Treatment Options
Non-surgical
- Immobilisation in a cast or splint for 6–12 weeks is appropriate for undisplaced fractures, especially those in the proximal or waist region.
- Repeat imaging is used to confirm healing before mobilisation.
- Smoking cessation and good nutrition aid bone repair.
Most stable fractures unite successfully with conservative treatment if diagnosed promptly.
Surgical
Surgery may be indicated if the fracture is displaced, unstable, or not healing with casting.
- Internal fixation with a headless compression screw allows accurate alignment and promotes faster healing.
- Bone grafting (from the radius or iliac crest) may be required for established nonunion or bone loss.
- Vascularised bone grafts are considered when blood supply to the proximal pole is compromised.
Surgery enables earlier mobilisation and reduces the risk of long-term stiffness, though postoperative rehabilitation is still essential.
Recovery & Follow-up
Healing time varies depending on the fracture site and blood supply.
- Distal fractures: usually heal within 6–8 weeks.
- Waist fractures: take around 8–12 weeks.
- Proximal pole fractures: may take longer, sometimes requiring surgical grafting.
Physiotherapy is important once immobilisation ends to restore motion and strength. Most patients regain near-normal wrist function, though stiffness and weakness can persist for several months.
Nonunion or avascular necrosis may lead to progressive wrist arthritis (Scaphoid Nonunion Advanced Collapse – SNAC wrist), sometimes requiring salvage procedures such as partial wrist fusion in chronic cases.
Follow-up appointments and repeat imaging ensure union and prevent late complications.
When to seek urgent help
Seek urgent assessment if wrist pain persists beyond a few days after a fall, particularly if localised on the thumb side, or if you experience swelling, clicking, or weakness that does not improve. After treatment, new pain, swelling, or reduced motion should be reviewed promptly to rule out delayed healing or hardware irritation.
Call 999 immediately or attend A&E if you have a new injury with loss of movement or sensation in the hand, rapidly spreading redness or swelling with fever, or sudden severe weakness.
Use NHS 111 for urgent same-day advice if your symptoms are getting quickly worse.
If you’re experiencing a scaphoid fracture or related symptoms, we can confirm the cause and tailor a plan – often starting with splints/hand therapy and exercises, with medicines, injections or surgery only where appropriate.
This page provides general information and is not a substitute for individual medical advice.
For emergencies (severe/new weakness, spreading infection, uncontrolled pain, significant injury) call 999, or use NHS 111 for urgent guidance.
Appointments:
- Self-pay patients can book without a GP referral
- Insured patients (Bupa, AXA, Aviva, Vitality, WPA, etc…) can book once authorised.
Clinics are available at:
- The Harborne Hospital – HCA, Birmingham
- Nuffield Health Wolverhampton Hospital
- The Priory Hospital, Birmingham
To book or ask a question, contact Vikki (Private Secretary):
☎ 07510 417479
✉ [email protected]