TFCC Tear (Triangular FibroCartilage Complex Injury)
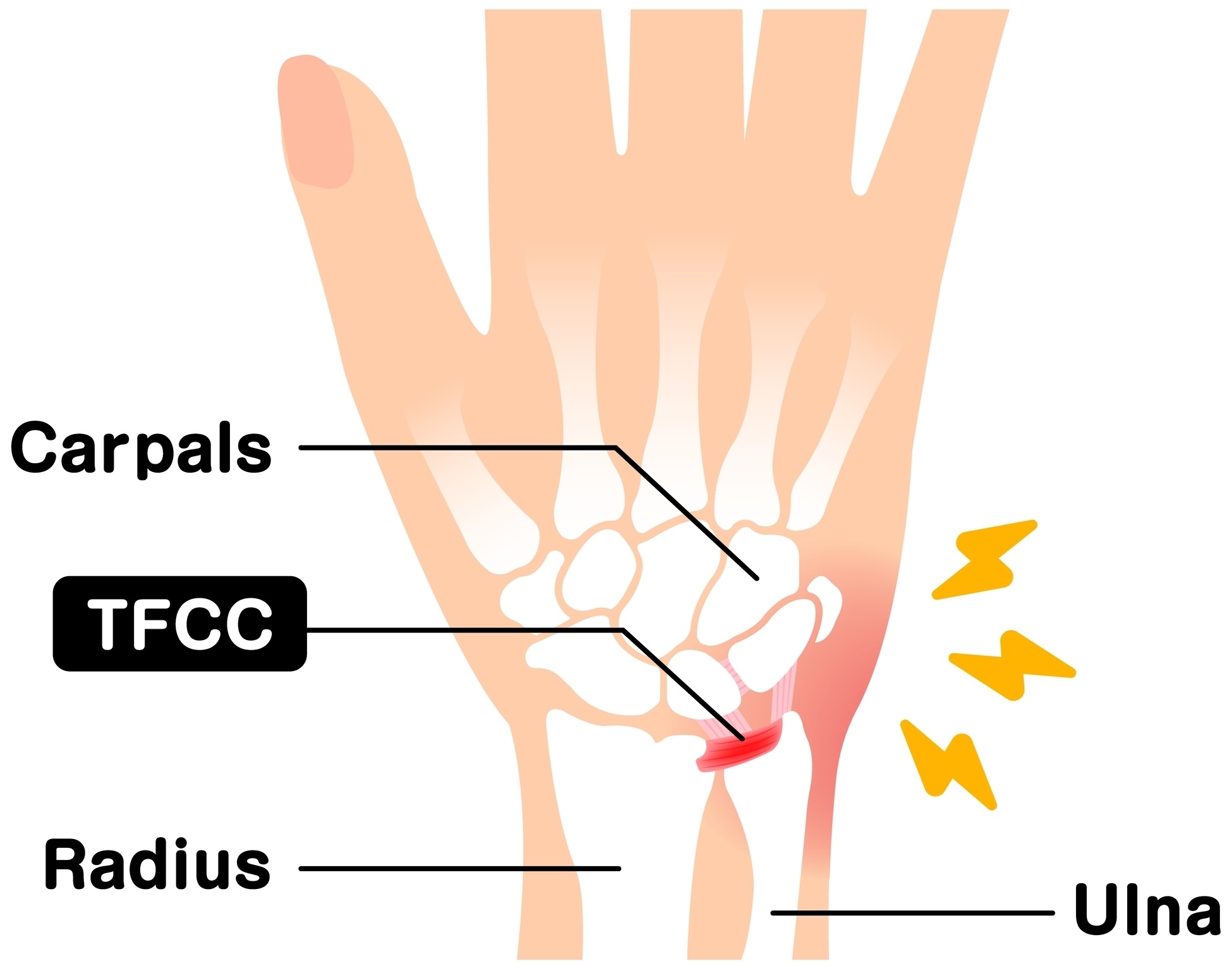
The Triangular FibroCartilage Complex (TFCC) is a specialised structure on the little-finger side of the wrist that stabilises the joint between the forearm bones and cushions the wrist during movement. A TFCC tear can result from trauma, such as a fall onto an outstretched hand, or from wear and tear over time i.e. degenerative. It typically causes pain on the ulnar (little finger) side of the wrist, often made worse by twisting or gripping. While some injuries settle with rest or splinting, others may require injection, arthroscopic repair, or bone shortening procedures to restore stability and function.
Common Symptoms
- Pain on the little-finger side of the wrist
- Discomfort when twisting the wrist (e.g. turning keys, opening jars)
- Clicking, catching, or a feeling of instability in the wrist
- Weakness when gripping
- Swelling or tenderness over the ulnar wrist
Typical Causes
TFCC tears may occur after a fall onto an outstretched hand, a sudden twisting injury, or repetitive loading of the wrist. Degenerative tears are common with age or in individuals with a naturally longer ulna bone (i.e. positive ulnar variance), which increases pressure on the TFCC. Sports such as tennis, golf, and gymnastics are frequent triggers due to repetitive wrist rotation.
Seek urgent help if
You experience sudden severe wrist pain with swelling or loss of rotation after a fall, or if the wrist feels unstable or “gives way” during movement. These may indicate a significant TFCC tear or associated ligament injury that needs early specialist assessment.
Call 999 for emergencies, or NHS 111 for urgent advice.
On this page:
Symptoms
Pain is typically located on the ulnar (little-finger) side of the wrist, just beyond the bony prominence at the end of the ulna. The discomfort often worsens with rotation, gripping, or weight-bearing through the wrist, such as pushing up from a chair.
Patients may describe clicking, grinding, or a feeling that the wrist is unstable. In some cases, pain develops gradually, especially in those with degenerative tears. Weakness and swelling are common, and the pain may persist even after minor activity. If the injury involves instability of the distal radioulnar joint (DRUJ), patients may also notice loss of forearm rotation.
Causes / Risk Factors
The TFCC acts as a complex stabiliser between the radius, ulna, and carpal bones. It includes cartilage, ligaments, and tendon attachments that absorb load and allow smooth wrist movement.
Risk factors and causes include:
- Trauma: fall onto an outstretched hand or sudden twisting injury
- Degenerative wear: gradual thinning of the TFCC with age
- Ulnar variance: longer ulna bone increases mechanical stress on the complex
- Repetitive strain: sports or occupations involving forearm rotation or forceful grip
- Arthritis: particularly ulnocarpal impaction or DRUJ degeneration
TFCC tears can occur in isolation or alongside other wrist injuries such as scaphoid fractures or distal radius fractures.
Investigations & Diagnosis
Diagnosis begins with a detailed clinical examination. Typical findings include tenderness over the ulnar fovea (just distal to the ulnar head) and pain during forearm rotation or ulnar deviation.
Investigations include:
- X-rays: to exclude fractures or assess ulnar variance.
- MRI scan: the gold standard for visualising TFCC tears and associated soft tissue damage.
- Wrist arthroscopy: both diagnostic and therapeutic – allows direct inspection and potential repair of the TFCC.
In some cases, dynamic fluoroscopy or CT scans may be used to assess subtle instability of the distal radioulnar joint.
Treatment Options
Non-surgical
Many TFCC tears, particularly minor or degenerative ones, can be managed without surgery.
- Rest and splinting: immobilisation in a wrist or forearm brace for 4–6 weeks to allow healing.
- Activity modification: avoiding heavy twisting, gripping, or weight-bearing.
- Corticosteroid injection: targeted injection into the TFCC region to reduce inflammation and pain.
- Physiotherapy: gradual strengthening and proprioceptive exercises once pain settles.
Surgical
Surgery is considered when symptoms persist despite conservative treatment or if there is clear mechanical instability. Options include:
- Arthroscopic debridement: trimming frayed tissue to relieve pain and improve movement, used for central degenerative tears.
- Arthroscopic or open repair: reattachment of torn ligaments, especially for peripheral or traumatic tears.
- Ulnar shortening osteotomy: for degenerative tears with positive ulnar variance to reduce pressure on the TFCC.
The appropriate procedure depends on tear type, chronicity, and associated instability.
Recovery & Follow-up
Recovery time varies depending on the severity and treatment method.
- Conservative treatment: most patients improve within 6–10 weeks.
- Arthroscopic debridement: allows early movement, with return to light activities in 3–4 weeks.
- TFCC repair: requires a longer rehabilitation period, with the wrist immobilised in a cast or splint for 6 weeks, followed by physiotherapy for 2–3 months.
Full return to sport or heavy manual work typically takes 3–6 months after repair. Long-term outcomes are generally excellent, though mild residual weakness or discomfort can persist, especially after degenerative tears.
When to seek urgent help
Seek urgent medical review if wrist pain worsens after treatment, if swelling or redness develops around the wrist, or if you experience sudden locking or loss of rotation. After surgery, increasing pain, discharge, or numbness should be assessed promptly to rule out infection or nerve irritation.
Call 999 immediately or attend A&E if you have a new injury with loss of movement or sensation in the hand, rapidly spreading redness or swelling with fever, or sudden severe weakness.
Use NHS 111 for urgent same-day advice if your symptoms are getting quickly worse.
If you’re experiencing ulnar sided wrist pain or related symptoms, we can confirm the cause and tailor a plan – often starting with splints/hand therapy and exercises, with medicines, injections or surgery only where appropriate.
This page provides general information and is not a substitute for individual medical advice.
For emergencies (severe/new weakness, spreading infection, uncontrolled pain, significant injury) call 999, or use NHS 111 for urgent guidance.
Appointments:
- Self-pay patients can book without a GP referral
- Insured patients (Bupa, AXA, Aviva, Vitality, WPA, etc…) can book once authorised.
Clinics are available at:
- The Harborne Hospital – HCA, Birmingham
- Nuffield Health Wolverhampton Hospital
- The Priory Hospital, Birmingham
To book or ask a question, contact Vikki (Private Secretary):
☎ 07510 417479
✉ [email protected]