Wrist Arthritis / Salvage Procedures
Wrist arthritis occurs when the smooth cartilage that lines the small wrist joints wears away, leading to pain, stiffness, and reduced function. It may develop after injury, repetitive strain, or as part of generalised osteoarthritis. When symptoms interfere with daily activities, various treatment options – from splints and injections to reconstructive or fusion (“salvage”) procedures – can help restore comfort and strength. Modern surgical techniques aim to relieve pain while preserving as much wrist movement as possible.
Common Symptoms
- Aching or sharp pain in the wrist, worsened by activity
- Morning stiffness or reduced range of motion
- Weakness and difficulty lifting or gripping objects
- Swelling or a feeling of grinding within the joint
- Loss of confidence in using the hand for everyday tasks
Typical Causes
Wrist arthritis may arise from previous trauma (such as a fracture or ligament injury), long-term overuse, or systemic conditions like rheumatoid arthritis. In many patients, arthritis follows a specific pattern. For example, after scaphoid fracture nonunion (scaphoid nonunion advanced collapse – SNAC wrist) or scapholunate ligament injury (SLAC wrist). Over time, cartilage loss leads to bone-on-bone contact, inflammation, and stiffness.
Seek urgent help if
The wrist becomes acutely swollen, red, and hot, particularly if you have a history of arthritis or recent surgery – this may indicate infection or acute inflammation needing immediate medical attention.
Call 999 for emergencies, or NHS 111 for urgent advice.
On this page:
Symptoms
The main symptom is pain, which may be dull and aching or occasionally sharp with movement. Stiffness, reduced motion, and weakness are common, making simple tasks such as opening jars, pushing up from a chair, or lifting cooking pans difficult. Some patients experience clicking, grinding (crepitus), or swelling around the wrist. Symptoms typically fluctuate, with flare-ups triggered by overuse or cold weather. As arthritis progresses, the wrist may lose flexibility and develop visible deformity.
Causes / Risk Factors
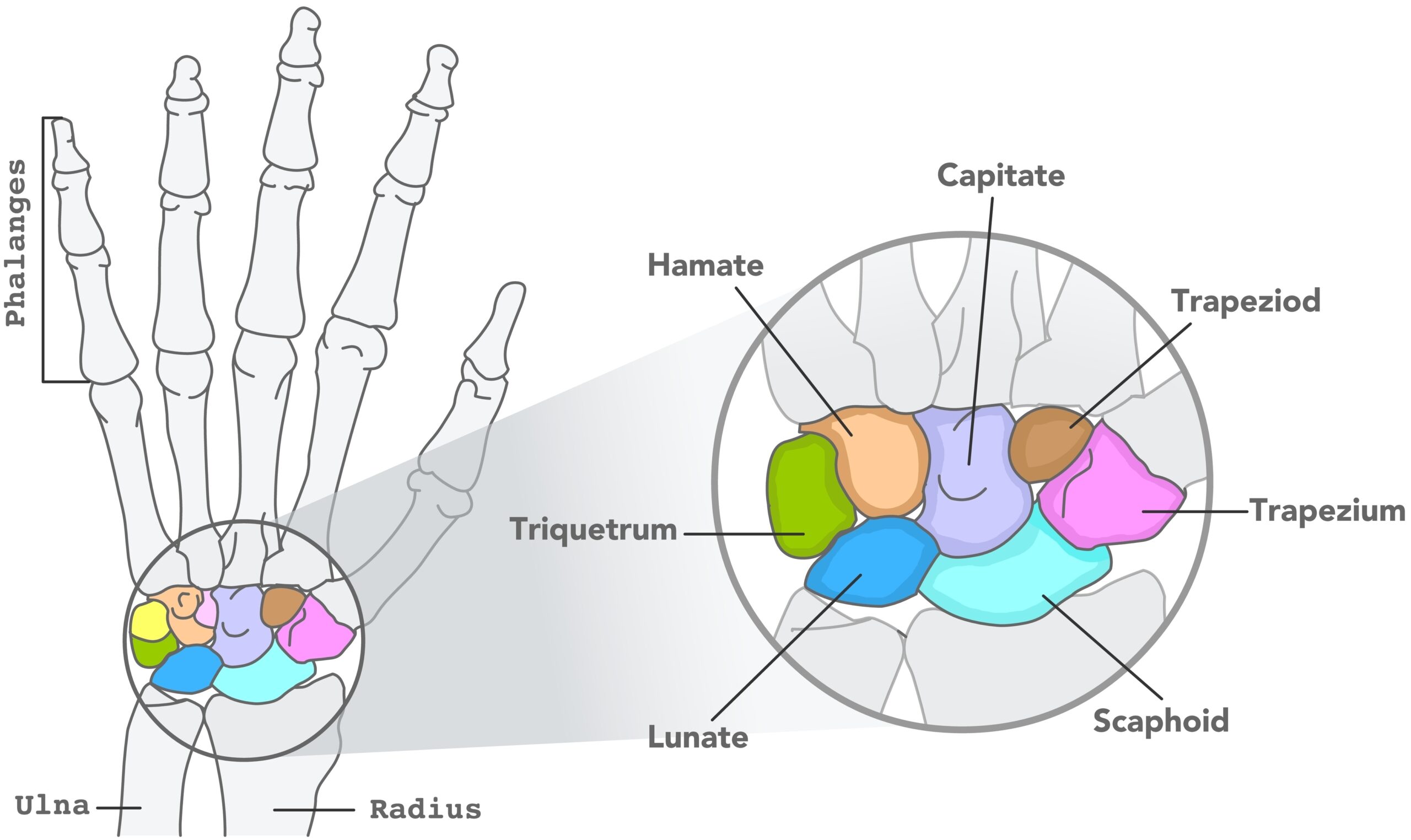
The wrist comprises multiple small bones and joints, making it susceptible to post-traumatic and degenerative changes.
Common causes include:
- Post-traumatic arthritis: following distal radius or scaphoid fracture, or ligament injuries such as scapholunate dissociation.
- Osteoarthritis: gradual cartilage wear with age or repetitive loading.
- Inflammatory arthritis: such as rheumatoid, psoriatic, or gouty arthritis.
- Avascular necrosis: collapse of carpal bones (e.g. Kienböck’s disease).
- Genetic or occupational factors: prolonged repetitive strain or vibration exposure.
Patterns such as SNAC (Scaphoid Nonunion Advanced Collapse) and SLAC (Scapholunate Advanced Collapse) describe predictable sequences of degenerative change and guide treatment planning.
Investigations & Diagnosis
Diagnosis involves careful clinical examination for tenderness, swelling, and range of motion.
Investigations may include:
- X-rays: to confirm joint-space narrowing, osteophytes, or bone collapse.
- CT scan: provides detailed three-dimensional assessment of bone alignment and arthritis pattern.
- MRI: useful in early or partial arthritis and for assessing adjacent soft tissue structures.
Blood tests may be ordered if an inflammatory cause is suspected. Identifying the pattern and severity of arthritis helps determine whether joint-preserving or fusion procedures are most appropriate.
Treatment Options
Non-surgical
- Activity modification and splints: reducing heavy or repetitive wrist use can alleviate pain.
- Analgesics and anti-inflammatories: help control pain and swelling.
- Corticosteroid injection: targeted relief of inflammation, often lasting several months.
- Physiotherapy: to maintain flexibility and strength, sometimes combined with occupational therapy for task adaptation.
Surgical
If pain persists despite conservative treatment, surgery may be indicated. The goal is to relieve pain while preserving function wherever possible.
Options include:
- Wrist denervation: selective division of sensory nerves to reduce pain while maintaining movement.
- Proximal Row Carpectomy (PRC): removal of the first row of carpal bones (scaphoid, lunate, triquetrum) to create a smooth, pain-free articulation. Suitable when midcarpal surfaces remain healthy.
- Four-corner fusion: fusion of the remaining carpal bones after scaphoid excision, offering stability with partial movement retention.
- Total wrist fusion (arthrodesis): used for severe, widespread arthritis; eliminates pain but sacrifices movement.
- Total wrist replacement (arthroplasty): preserves some motion and is an option for low-demand patients with inflammatory arthritis.
Your surgeon will discuss which procedure best matches your symptoms, wrist pattern, and functional goals.
Recovery & Follow-up
Recovery time depends on the type of treatment.
- After injection or splinting, improvement may occur within days, with effects lasting several months.
- Following PRC or four-corner fusion, the wrist is immobilised in a cast for 6–8 weeks before physiotherapy begins.
- Light use often resumes by 8–10 weeks, with ongoing improvement for up to 6 months.
- Total wrist fusion provides reliable pain relief and strength but no wrist flexion or extension; most patients adapt well to this limitation.
Physiotherapy is crucial for maintaining hand and finger motion. Regular follow-up and imaging confirm bone healing and ensure optimal functional recovery.
When to seek urgent help
You should seek urgent review if you develop increasing pain, swelling, or discharge at the surgical site, sudden loss of wrist or finger movement, or new numbness or tingling. After an injection, persistent redness or warmth may signal infection or an adverse reaction requiring prompt treatment.
Call 999 immediately or attend A&E if you have a new injury with loss of movement or sensation in the hand, rapidly spreading redness or swelling with fever, or sudden severe weakness.
Use NHS 111 for urgent same-day advice if your symptoms are getting quickly worse.
If you’re experiencing wrist pain or related symptoms, we can confirm the cause and tailor a plan – often starting with splints/hand therapy and exercises, with medicines, injections or surgery only where appropriate.
This page provides general information and is not a substitute for individual medical advice.
For emergencies (severe/new weakness, spreading infection, uncontrolled pain, significant injury) call 999, or use NHS 111 for urgent guidance.
Appointments:
- Self-pay patients can book without a GP referral
- Insured patients (Bupa, AXA, Aviva, Vitality, WPA, etc…) can book once authorised.
Clinics are available at:
- The Harborne Hospital – HCA, Birmingham
- Nuffield Health Wolverhampton Hospital
- The Priory Hospital, Birmingham
To book or ask a question, contact Vikki (Private Secretary):
☎ 07510 417479
✉ [email protected]